In a paper recently published in the Proceedings of the National Academy of Sciences of the United States of America, Dr. Bruce Vallance (CH.I.L.D. Foundation Endowed Chair for Research in Pediatric Gastroenterology) and the rest of his research team found that sialic acid, a sugar derived from intestinal mucus, fuels pathogenic disease-causing bacteria. “This means that in the future, we can potentially target this sugar or how pathogens sense it, to prevent clinically important disease,” stated Dr. Vallance.
Dr. Bruce Vallance
Besides causing infection and disease, pathogenic and similar dangerous bacteria can be found in the intestines of some patients who suffer from inflammatory diseases such as IBD. Such bacteria may start out being harmless, but as the inflammatory diseases progress, the bacteria can change over time and worsen disease.
According to Dr. Vallance, “You start off with IBD, your microbes change, they start digging their way into the cells lining your gut, causing more inflammation, and that may be one reason why IBD becomes chronic. Specific nutrients such as sialic acid or other sugars might be Achilles heels for them in terms of things you could target to remove dangerous bacteria from the intestine.”
Thus, targeting sialic acid could be a way to prevent life-threatening diarrheal diseases in children in developing countries, as well as help treat patients with IBD and other inflammatory diseases.
Dr. Vallance and his team are now examining the role other sugars in the gut might play in feeding pathogenic bacteria. Additionally, they are looking for resident good bacteria (probiotics) that could out-compete the dangerous bacteria, stealing the sugars away from them.
They also plan to explore potential interactions between resident and pathogenic bacteria. The latter can’t access the sugars on their own and thus, some of the typically harmless resident bacteria must serve as accomplices.
A better understanding of these interactions could provide new ways to block pathogenic disease-causing bacteria.
Over the past years the CH.I.L.D. Foundation has worked hard to raise funds for important research. Since the very beginning our mission has remained clear – to find a cure for pediatric Crohn’s Disease, Ulcerative Colitis and Liver Disorders. Our Network works tirelessly, and with great successes to get us closer to this goal. In just the past year, these researchers have achieved truly remarkable feats and remain on the forefront of the field. The following are some of the exciting achievements by our researchers in the past year, we are grateful for their work to help those forgotten children and their families.
Dr. Bruce Vallance
Bruce Vallance and Eytan Wine received the CIHR microbiome grant totaling $2 Million over four years. Their proposal “Role of Microbes in the pathogenesis of Pediatric IBD: From discovery, through causation, to novel treatments” ranked #1 out of 7 teams. This extraordinary team will study the complicated role of microbes and gut microbiomes in pediatric Inflammatory Bowel Disease. This focus proves promising and the CH.I.L.D. Foundation is grateful and excited to be involved in such ground-breaking research.
Dr. Amanda Ricciuto
Dr. Amanda Ricciuto was awarded the 2020 PRO-KIIDS pilot award. Only one grant was awarded by PRO-KIIDS, which Dr. Ricciuto won with her project “Serum Cytokine Profiles to Predict Anti-TNF Responsiveness in Pediatric Inflammatory Bowel Disease”. Dr. Ricciuto has focused her PhD research on pediatric IBD/ liver disease, specializing in primary sclerosing cholangitis. Dr. Ricciuto contributes greatly to her field of pediatric gastroenterology, and this award showcases her work as an example of innovation and dedication in the field.
Dr. Anne Griffiths
Dr. Anne Griffiths received the 2019 Shwachman award, the highest honour awarded by NASPGHAN (North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition). This award is given to an individual who has made “major, lifelong scientific or education contributions to the field of pediatric gastroenterology, hepatology, or nutrition in North America”. As the co-lead for Sickkids IBD Centre and the Principal Investigator for the Canadian Children Inflammatory Bowel Disease Network of the CH.I.L.D. Foundation, Dr. Griffiths is not only carving out extensive space for research in the field of pediatric Gastroenterology, but remains in close connection with the CH.I.L.D. Foundation.
Here are just a few of the publications from these amazing scientists. These studies fill in knowledge gaps in our current approach to treating these diseases and carve pathways for a cure:
Amanda Ricciuto, Jasbir Dhaliwal, Thomas D Walters, Anne M Griffiths, Peter C Church, Clinical Outcomes With Therapeutic Drug Monitoring in Inflammatory Bowel Disease: A Systematic Review With Meta-Analysis, Journal of Crohn’s and Colitis, Volume 12, Issue 11, November 2018, Pages 1302–1315, https://doi.org/10.1093/ecco-jcc/jjy109
Griffiths, Anne,. et al. “Genome-wide meta-analysis increases to 71 the number of confirmed Crohn’s disease susceptibility loci”. Nat Genet 42, 1118–1125 (2010). https://doi.org/10.1038/ng.717
Griffiths, Anne,. et al. “The Treatment-Naïve Microbiome in New-Onset Crohn’s Disease” Cell Host & Microbe Resource, vol. 15, pp. 382-392., doi: doi.org/10.1016/j.chom.2014.02.005
Vallance, Bruce, et al. “Cutting Edge: Intestinal Mucus Limits the Clonal Deletion of Developing T Cells Specific for an Oral Antigen.” The Journal of Immunology, vol. 205, no. 2, 2020, pp. 329–334., doi:10.4049/jimmunol.1900687.
Vallance, Bruce, et al. “Intestinal Epithelium-Specific MyD88 Signaling Impacts Host Susceptibility to Infectious Colitis by Promoting Protective Goblet Cell and Antimicrobial Responses.” Infection and Immunity, vol. 82, no. 9, 2014, pp. 3753–3763., doi:10.1128/iai.02045-14.
Vallance, Bruce, et al. “Control of Intestinal Homeostasis, Colitis, and Colitis-Associated Colorectal Cancer by the Inflammatory Caspases.” Immunity, vol. 32, no. 3, 2010, pp. 367–378., doi:10.1016/j.immuni.2010.02.012.
If you’d like to know more about our incredible researchers, find more info here:
Dr. Amanda Ricciuto: http://www.sickkids.ca/AboutSickKids/Directory/People/R/Amanda%20Ricciuto.html
Dr. Bruce Vallance: https://www.bcchr.ca/bvallance
Dr. Anne Griffiths: http://www.sickkids.ca/AboutSickKids/Directory/People/G/Anne-Griffiths.html
Modern medicine is nothing short of a miracle. Whether it’s vaccines as a child or complicated surgeries and procedures later in life, there are few people who do not owe some portion of their health to medical ‘cures’. Countless amounts of time, effort, and resources goes into these life saving solutions. But some work better than others, and many offer patients truly difficult choices.
A child taking prescription medication
Steroids and corticosteroids (like prednisone) are perhaps the most common treatment for Crohn’s disease across all ages. Steroids are used to suppress the inflammation of the gastrointestinal tract, and are the most effective method of treatment to date. They relieve many symptoms of Crohn’s Disease within a matter of days or weeks, and are usually taken as a tablet.
If steroids are so effective and easy to take, why then are they not considered a Crohn’s Disease miracle drug? Have we solved the crisis? Unfortunately, like many things in life, something this good doesn’t come without significant downsides. Steroids come with a long list of terrible side effects ranging from short term and cosmetic to long term and debilitating.
Would you take a pill that listed common side effects of the following?
Acne
Redness of the face
“Chubby cheeks”
A tendency to bruise easily
Fluid retention
Increased appetite
Weight gain
Bone loss
Increased blood pressure
Increased susceptibility to infections
Mood swings
Depression
In uncommon cases steroid use can cause muscle weakness and psychosis. This is why steroids are often used as a short term solutions, but this short term solution often turns into a long term solution when symptoms become unmanageable. Troublingly, in children prolonged steroid use leads to stunted growth, with most pediatric cases averaging a short or much shorter height than most adults. This is because prolonged use of steroids- like treatment of pediatric Crohn’s patients- also results in the following problems in addition to those listed above:
Osteoporosis
Cataracts
High blood pressure
Steroid-induced diabetes
This is just one reason why lifelong diseases like IBD, Crohn’s, etc. are so frustrating. Not only are the symptoms terrible, but often the treatments are not actually solutions but gateways into other problems. For example, steroids often conflict with other medications and cause complications among other treatments. These complications and symptoms compound into a tangled mess of diagnoses, treatments, treatments for the symptoms caused by the treatments, and problematic interactions between symptoms and side effects.
No two Crohn’s patients are alike. For some, steroids are akin to a cure and Crohn’s symptoms are easily managed. However for the majority, steroid use is simply the beginning of a lifetime cycle of treatments and symptoms. These trade-offs are near impossible to navigate, with so many unanswered questions, side effects that are yet to be discovered, and solutions that simply do nothing but complicate things further.
This highlights our need for a cure, not simply a treatment, for Crohn’s Disease. We need a solution that tackles the problem without trading Crohn’s symptoms for steroid side effects. We remain dedicated as ever to finding a cure for these forgotten children.
“Crohn’s Disease Treatment.” NHS Crohn’s Treatment, National Health Society, 4 Apr. 2018, www.nhs.uk/conditions/crohns-disease/treatment/.
Heuschkel, Robert B, et al. “Enteral Nutrition and Corticosteroids in the Treatment of Acute Crohn’s Disease in Children.” Journal of Pediatric Gastroenterology and Nutrition, vol. 31, no. 1, 2000, pp. 8–15., doi:10.1097/00005176-200007000-00005.
Lahad, A., & Weiss, B. (2015). Current therapy of pediatric Crohn’s disease. World journal of gastrointestinal pathophysiology, 6(2), 33–42. https://doi.org/10.4291/wjgp.v6.i2.33 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4419092/#__sec4title
Sawczenko
A, Ballinger AB, Savage MO, Sanderson IR. Clinical features affecting
final adult height in patients with pediatric-onset Crohn’s disease. Pediatrics. 2006;118(1):124-129. doi:10.1542/peds.2005-2931 https://pubmed.ncbi.nlm.nih.gov/16818557/
A
child’s life should be one of innocence, play, learning, and family.
However, this is simply not the case for children with IBD. Often, their
play is halted short by hospital visits, surgeries, pain, and poor health. For these children who have to swap out play dates with painkiller and basketballs with blood tests, they miss out on critical time with friends, family, and even just simply feeling well.
I recently came across a picture book called “A Bridge to Experience” written and illustrated by a 12 year old Crohn’s patient. The young author uses the fictional main character ‘Julie’ to explore her struggle with Crohn’s. In the honest and straightforward way that only a 12 year old can write, the writer heartbreakingly chronicles Julie’s trajectory from a happy young woman with a paper route and upcoming basketball championship to a survivor of major surgery and uncounted painful hospital visits in a matter of days.
I
can only imagine how “A Bridge to Experience” helped other children
understand more about the experiences of pediatric IBD and Crohn’s
patients. But as an adult, reading this short 31 page novel was eye opening and heart breaking. Julie’s thoughts along her journey are brutally honest and lay bare the reality of the emotions of an ill child stuck in the hospital.
She recounts her first night in the hospital: “…she
thought it was a dreary place where people die, and didn’t want
anything to do with it, but she didn’t really control her future.” and being hooked up to all sorts of tubes and mechanisms.
She somewhat humorously tells of being “…bored out of her mind and desperately looking for something to do…” while waiting for doctors, nurses, and answers.
She recalls feeling helpless and scared, “…exploding with questions that needed to be answered.”
And, most difficult to read, are the times when she talks of letting out “blood-curdling” screams, the pain she felt during procedures, and feeling “…her eyes almost close forever…”.
Reading this book felt, truthfully, disturbing. It’s upsetting to think about a child writing these words- especially from personal experience. I think our discomfort with the subject is both good and bad. We should never be comfortable with children being in pain. But, because it is so uncomfortable it is easy to ignore these forgotten children, to push them out of our worry and assume that the problem is being taken care of.
We cannot ignore these children. Canada has among the highest rates in the world- and it is inexplicably and dramatically rising. 25% of these are children.
“A Bridge to Experience” is the story of just one of these children, the tale is replicated by hundreds of thousands of children. So for children like Julie who had their childhoods stolen by pain
and hospitals with no cure or end in sight, we must continue fighting
for a cure. So that no child ever has to write a book like this again.
References:
Anonymous. “A Bridge to Experience”, Parsons Publishing Co, 1993.
Gilaad
G Kaplan, MD, MPH, Charles N Bernstein, MD, Stephanie Coward, MSc,
Alain Bitton, MD, Sanjay K Murthy, MD, MS, Geoffrey C Nguyen, MD, PhD,
Kate Lee, MBA PhD, Jane Cooke-Lauder, MBA, DM, CMC, Eric I Benchimol, MD, PhD, “The Impact of Inflammatory Bowel Disease in Canada 2018: Epidemiology”, Journal of the Canadian Association of Gastroenterology, Volume 2, Issue Supplement_1, February 2019, Pages S6–S16, https://doi.org/10.1093/jcag/gwy054
Every single person does it nearly every day, but going to the bathroom is still one of the most taboo subjects in society. But
we need to eat to live, and we need to poop to eat- so your bowel
movements are actually crucial insights into the healthiness of the
processes happening in your body!
While it might be uncomfortable to talk about the stinky things that go on between you and your toilet, discussing it with others – especially doctors – is crucial to your wellbeing. How would you know if your bowel movements are abnormal if you don’t know what ‘normal’ is? Healthcare professionals even recommend keeping a ‘poop journal’ in order to better track what goes into your body, what it does, and how it comes out.
In fact, many cultures have embraced feces as an important, even cherished health and wellness tactic. In many part of Asia, for example, poop is more normalized with ‘poop museums’, mascots, restaurants and even poop shaped food.
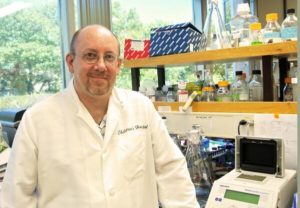
While these whimsical portrayal of poop may seem childish and silly, they show an underlying social norm that thinking about your bowel movements is good- encouraged even. And there may be great benefits to destigmatizing feces; Asian countries have far lower rates of IBD than western countries, especially North America.
IBD Rates by Country (Alatab et al.)
For patients with IBD, bowel movements can take over their health and lives. Going to the bathroom is not just a yucky chore, but a painful and draining task. While different types of IBD can present with different symptoms the most common are watery diarrhea, blood in the stool, painful cramping in the lower abdomen and excruciating bowel movements. These symptoms are not normal and often hinder day to day life. Yet patients often feel that they cannot talk about their experience with those closest to them, because it is ‘icky’.
Inflammatory Bowel Disease is a terrible one with no cure. Managing these symptoms is difficult enough without feeling as if you can’t speak about the problems with friends and family. This can be isolating, lonely, and scary.
We all poop. It might not be the most pleasant constant in our lives, but it remains a constant nonetheless. So let’s talk about it more! Communication is important, especially when it comes to our health. Avoiding the subject will only lead to more uncertainty
and less research. So next time you poop, be grateful to your body for
allowing you to do so and make sure to carefully track any
irregularities and report them to your doctors
And, most importantly, reach out to your friends and family suffering with IBD and offer support. 1 in every 200 North Americans has been diagnosed with IBD, which means that you probably know someone even if you don’t think you do! Let’s all be a little more comfortable with bowel movements- it will only help.
References:
Alatab, Sudabeh, et al. “The Global, Regional, and National Burden of Inflammatory Bowel Disease in 195 Countries and Territories, 1990–2017: a Systematic Analysis for the Global Burden of Disease Study 2017.” The Lancet Gastroenterology & Hepatology, vol. 5, no. 1, 2020, pp. 17–30., doi:10.1016/s2468-1253(19)30333-4.
Loftus, Edward V Jr. “Update on the Incidence and Prevalence of Inflammatory Bowel Disease in the United States.” Gastroenterology & hepatology vol. 12,11 (2016): 704-707.
McGlotten , Shaka. “Poop Worlds: Material Culture and Copropower (or, Toward a Shitty Turn).” S&F Online, sfonline.barnard.edu/traversing-technologies/poop-worlds-material-culture-and-copropower-shaka-mcglotten-scott-webel/.
Weyrauch, Emily, and Elana Vlodaver. “Poop Culture.” The Bowdoin Orient, 24 Oct. 2014, bowdoinorient.com/bonus/article/9601.
Full hospitals are bad if you rely on regular visits
By: Hannah Stevenson
At
7 PM, many cities around the world erupt in cheers for the healthcare
heroes that fight every day on the front lines of this pandemic. Most of
us live our lives avoiding hospital visits- usually a sign that
something has gone very wrong. For doctors, nurses, and healthcare
workers hospitals are a workplace and an everyday occurrence. Amidst all
the fear, uncertainty, and challenges brought about by the Coronavirus,
people who rely on the hospital and its staff must also make sacrifices
as doctors and nurses are needed to fight this pandemic.
Those
with chronic illnesses- like IBD, Crohn’s, and liver disorders- often
rely on frequent doctor appointments, hospital visits, and even surgery
and testing. During this pandemic, many of these are limited, postponed,
or cancelled, leaving IBD patients waiting through uncomfortable
symptoms or ill-managed diseases.
The
most pressing risk to IBD patients is lack of access to vital
medications, particularly immunosuppressants. Immunosuppressants are key
to managing many patients’ most terrible symptoms, but also leave the
patient with a depleted- or suppressed- immune system. While early
preliminary studies show that IBD patients are not necessarily at any
higher risk for contracting COVID-19, there are strong associations
between IBD and Immunodeficiency as well as Autoimmune Disorders. Those
with Immunodeficiency, or immunocompromised people, have depleted or
inefficient immune systems, leaving them much more vulnerable to
coronavirus and its symptoms. Those who are immunocompromised must take
great precautions, many cannot risk allowing themselves or household
members to leave their own house- even receiving deliveries pose threat
of infection. Furthermore, immunocompromised people who have contracted
illnesses must fight much harder to combat them, and often requiring
hospital visits and special equipment.
For
children with IBD, this can mean being cooped up indoors all day- often
while coping with painful and uncomfortable symptoms. Imagine being a
child who wants to play with their friends in the sunshine, but instead
is ill and indoors for months!
At
the CH.I.L.D. Foundation, we have spent 25 years working with amazing
researchers, doctors, nurses, and healthcare professionals. We know how
hard they work, how often they put themselves at risk, and how
selflessly they strive to heal others. We are so grateful for them;
especially as recent events have highlighted the importance of good
health and those who work for it.
Finding a cure to IBD has
never been more important, or more possible. To all of our supporters,
friends- and especially healthcare partners- be safe and show support to
those who need it most.
Studies cited:
Glocker, Erik, and Bodo Grimbacher. “Inflammatory Bowel Disease: Is It a Primary Immunodeficiency?” Cellular and Molecular Life Sciences, vol. 69, no. 1, 2011, pp. 41–48., doi:10.1007/s00018-011-0837-9.
Snook, JA, et al. “The Association of Autoimmune Disorders with Inflammatory Bowel Disease.” QJM: An International Journal of Medicine, 1989, doi:10.1093/oxfordjournals.qjmed.a068372.
Danese, S., Cecconi, M. & Spinelli, A. Management of IBD during the COVID-19 outbreak: resetting clinical priorities. Nat Rev Gastroenterol Hepatol (2020). https://doi.org/10.1038/s41575-020-0294-8
Grace McCarthy was a highly successful businesswoman who opened her first
flower shop at 17 years of age and built it into five flourishing shops. Then
she decided to take on a public role for the next three decades. She was
a Vancouver Parks Commissioner, MLA and cabinet minister, serving as Deputy
Premier with several portfolios, including economic development, provincial
secretary, human resources and tourism.
She initiated Canada’s first toll-free Help Line for abused children;
successfully lobbied governments to enable women to own property without a male
guarantor; founded Canada’s first school of floral design, initiated the
Vancouver Trade & Convention Centre, established Canada’s first linear
parkway and SkyTrain, and initiated B.C.’s first film promotion office.
Retiring from public life, Grace McCarthy turned her attention to raising
funds for research to help children with Crohn’s Disease and Ulcerative
Colitis. She was a founder of the CH.I.L.D. Foundation, envisioning a
Canada-wide Network for Children with Inflammatory Bowel Diseases (IBD)
connecting doctors, researchers and families for the first time in Canada.
Grace McCarthy left an indelible mark on our entire province and we will
remember her kindness in making a difference in all our lives.
Grace was predeceased by her dearly beloved son Calvin in 2009, and will be
dearly missed by Raymond, her husband of sixty-nine years and by her daughter
Mary (Barry Parsons), her Grandchildren: The Reverend Canon Christopher Parsons
(Anke), Dr. Matthew Parsons (Mary), Shannon Parsons (Thomas Ernst), four
great-granddaughters: Hannah, Lucia, Bronwyn and Penny, and niece Lynne Nielsen
(Finn) and family.
CANADIAN CHILDREN INFLAMMATORY BOWEL DISEASE NETWORK:
A Joint Partnership of the CH.I.L.D. Foundation and the Canadian Institute of Health Research
The Canadian Children Inflammatory Bowel Disease Network: A Joint Partnership of the CH.I.L.D. Foundation and the Canadian Institute of Health Research has commenced its operations. The network leadership has submitted their response to the issues identified by the International Peer Review Panel in the spring of 2013 and that response has been reviewed favourably by the same international peer review panel members on September 26, 2013.
A Network Advisory Committee has been established to guide the network’s start-up and growth phase and offer advice on the most efficient and effective governance and leadership mechanisms for the network to use. The role of the Advisory Committee is to provide advice to the network leadership team and the funder organizations (the CH.I.L.D. Foundation and CIHR-INMD) on the required strategies, structures, and processes to further the network’s achievement of its strategic goals.
CCIBD Network Advisory Committee
Together with representatives from the CH.I.L.D. Foundation and CIHR. the inaugural meeting of the Network Advisory Committee will be held in Vancouver on October 19, 2013. The CH.I.L.D. Foundation is most appreciative of the Advisory Committee’s volunteer assistance and guidance.
Cathleen Morrison, Chair. Cathleen’s life work has been rooted in the charitable and voluntary sector. Cathleen led Cystic Fibrosis Canada for thirty years as Chief Executive Officer, during a time of remarkable growth and change, until her retirement in 2011. She is a member of the Board of Directors of Friends of Canadian Institutes of Health Research, and an Honourary Life Member of Research Canada – An Alliance for Health Discovery, having served as a Board member of the Canadian Bacterial Diseases Network, and as Chair of the National Voluntary Health Agencies Committee.
Neelu Chauhan, BSc, LLB, is a Labour Relations Consultant at British Columbia Institute of Technology, providing labour relations advice, service and support to management regarding the interpretation, administration and application of collective agreements in multi-union, public sector environments. An advocate for patients with Crohn’s Disease and Ulcerative Colitis, she has been a Member, Research Ethics Board, BCIT, and Member, Editorial Advisory Committee, Peopletalk Magazine, relating to wellness in the workplace.
Brett Finlay, OC, OBC, PhD, is a Professor in the Michael Smith Laboratories, and the Departments of Biochemistry and Molecular Biology, and Microbiology and Immunology at the University of British Columbia. By combining cell biology with microbiology, he has been at the forefront of the emerging field called Cellular Microbiology, making several fundamental discoveries in this field. He is well recognized internationally for his work, particularly as Director, SARS Accelerated Vaccine Initiative. He serves on several editorial and advisory boards, including the CH.I.L.D. Foundation Scientific Research Advisory Council, and is a strong supporter of communicating science to the public.
Claudio Fiocchi, MD, is a senior researcher in the department of pathobiology of Lerner Research Institute of Cleveland Clinic. He is also the Director of IBD and Vice Chairman of Research for the Department of Gastroenterology and Hepatology in the Digestive Disease Institute of Cleveland Clinic. His many awards include the Crohn’s and Colitis Foundation of America’s Janowitz Lifetime Achievement Award in Inflammatory Bowel Disease.
Peter Margolis, MD, PhD, is Professor, Pediatrics and Director of Research at the James M. Anderson Center for Health System Excellence at Cincinnati Children’s Hospital Medical Center. His work encompasses the application and study of quality improvement methods in a broad range of areas including primary and sub-specialty care, communities and public health settings to improve the health outcomes of children, families and communities. He is principal investigator on an NIH Roadmap transformative research grant on redesigning systems for chronic illness care.





 Foundation and the Canadian Institute of Health Research has commenced its operations. The network leadership has submitted their response to the issues identified by the International Peer Review Panel in the spring of 2013 and that response has been reviewed favourably by the same international peer review panel members on September 26, 2013.
Foundation and the Canadian Institute of Health Research has commenced its operations. The network leadership has submitted their response to the issues identified by the International Peer Review Panel in the spring of 2013 and that response has been reviewed favourably by the same international peer review panel members on September 26, 2013.

















